
For years, MASLD was often discussed primarily as a disease of fat accumulation in the liver. But clinically, the more important question is usually not whether fat is present. It is whether the liver is actively being injured and whether the disease is progressing.
That distinction matters because patients behave very differently over time. Some individuals live with steatosis for decades without major progression, while others move relatively quickly toward steatohepatitis, fibrosis, or cirrhosis. The amount of liver fat alone does not fully explain that difference.
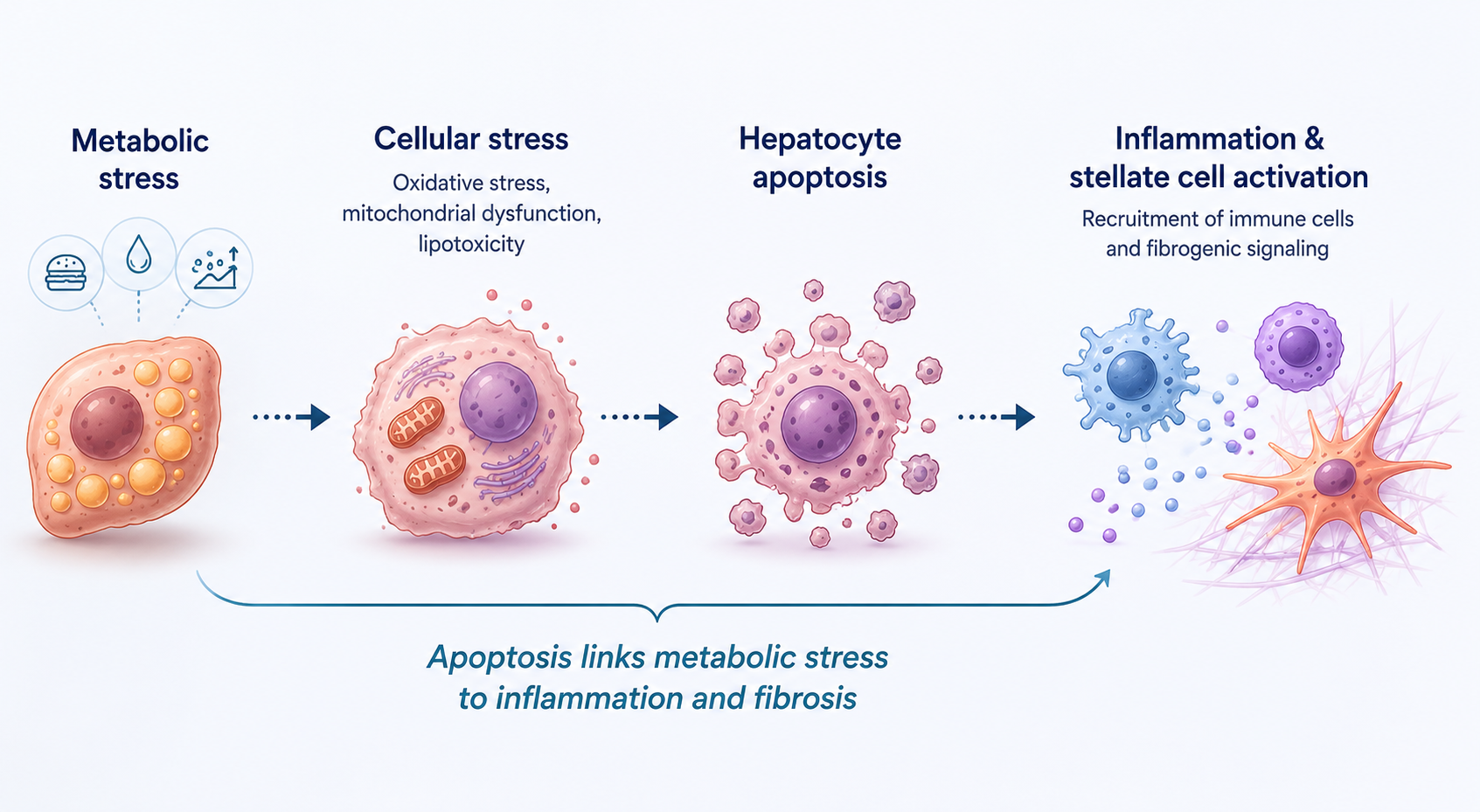
One of the processes increasingly believed to sit at the center of progression is hepatocyte apoptosis.
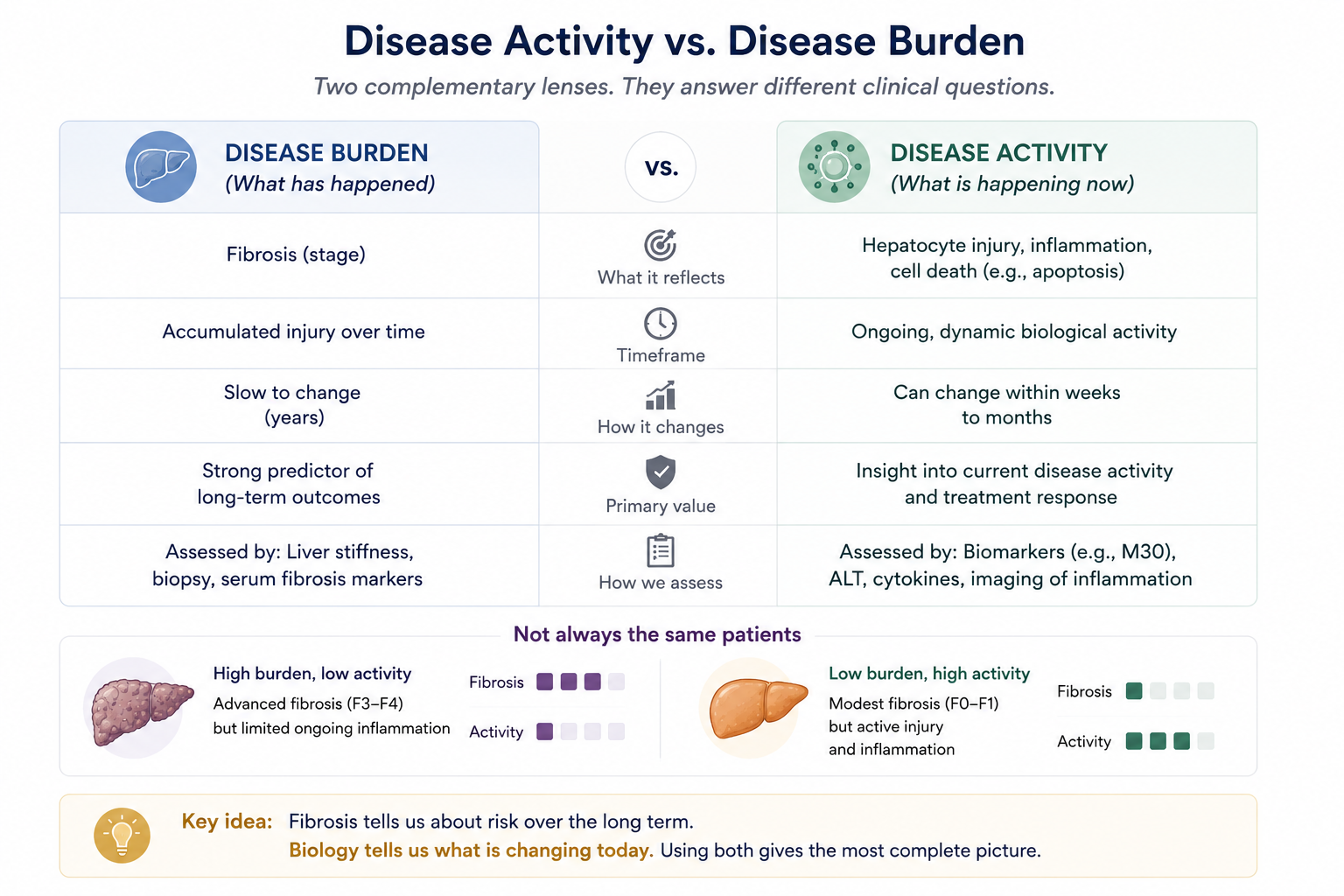
This shift in focus is important because hepatology has traditionally relied heavily on structural assessments, particularly fibrosis. Fibrosis remains enormously important prognostically. It predicts liver-related outcomes, decompensation risk, and mortality better than almost anything else we measure routinely.
But fibrosis also reflects accumulated injury. It does not always tell us much about what the liver is doing biologically today.
That becomes especially relevant now that pharmacological therapies are entering routine practice. If a patient starts treatment, clinicians do not want to wait years for fibrosis to slowly change before deciding whether the underlying disease activity is improving.
In practice, this limitation already shows up constantly. Patients with clearly active MASH may have only mildly elevated ALT levels. Liver enzymes fluctuate substantially between visits. Some patients show improvements in steatosis on imaging while inflammatory injury appears to persist underneath. Even liver stiffness can remain relatively stable despite meaningful biological improvement occurring earlier in the disease process.
This is part of the reason apoptosis biomarkers have continued to attract interest. They are attempting to measure something fundamentally different from fibrosis: active hepatocyte injury occurring in real time.
Why Apoptosis Biomarkers Became Interesting
One of the most studied biomarkers in this area is keratin 18 (K18). K18 is highly expressed in hepatocytes, and during apoptosis it is cleaved by activated caspases into specific fragments that are released into circulation. The M30 Apoptosense® ELISA detects these caspase-cleaved K18 fragments and therefore reflects apoptotic hepatocyte death.
What made apoptosis biomarkers interesting was not simply that they correlated with disease severity. Many biomarkers do that. The more interesting possibility was that they might provide insight into ongoing disease activity before structural changes become measurable.
Over the past two decades, elevated M30 levels have repeatedly been associated with hepatocyte ballooning, lobular inflammation, higher NAFLD Activity Scores (NAS), and more progressive fibrotic disease.
At the same time, the field has also learned that the biology is more complicated than many initially hoped.
M30 is clearly not a perfect discriminator, particularly in intermediate disease where biological overlap between patient groups is substantial. Some studies have shown stronger predictive performance than others, and its utility depends heavily on patient population and clinical context.
Still, the underlying rationale remains compelling. The liver can appear relatively stable structurally while remaining biologically active underneath. Apoptosis biomarkers are interesting because they attempt to capture that active biology directly.
Looking Ahead
MASLD management is gradually moving away from a purely descriptive model toward a more mechanistic one. The field is no longer asking only how much fibrosis is present, but increasingly what biological processes are actively driving progression in a given patient.
Apoptosis is one of those processes.
Whether apoptosis biomarkers ultimately become part of routine longitudinal monitoring remains uncertain, and there are still important questions around standardization, interpretation, and clinical integration. But the broader direction of the field is becoming increasingly clear: hepatology is moving toward understanding dynamic disease biology rather than relying exclusively on static structural endpoints.
That shift is probably necessary. Because in many patients, the biology changes long before the scar tissue does.
In the next article, we will look more closely at how apoptosis biomarkers such as M30 have been used in lifestyle intervention studies, including diet, weight loss, and exercise programs in patients with MASLD.